Background: Periventricular and Intraventricular processes are life-threatening conditions because of their propensity to obstruct Cerebrospinal fluid pathways and to compress highly functional and vital structures. There are deep-seated lesions requiring rigorous microsurgical technic for their resection. Methods: We retrospectively analyzed the profile and outcome of Periventricular and intraventricular processes operated by the same author since his return in his country in 2015, after graduated abroad in WFNS Rabat training center program 2023. Result: We defined 15 patients operated over 8 years. There were 4 processes in lateral ventricle (26.6%), 1 in third ventricle (6.6%), 2 thalamus processes (13.3%), 4 in fourth ventricle (26.6%) and finally 4 in cerebellar hemisphere and violating the fourth ventricle (26.6%). Various surgical approaches were used, such as contralateral interhemispheric transcallosal, classical interhemispheric transcallosal, Subfrontal transbasal translamina terminalis, Frontal Transcortical, Temporal trans T2, ventriculoperitoneal shunting, endoscopy, cerebellar transcotical approach and Telovelar approach. Surgical procedure duration was more than 10 hours in 12 cases (80%) and one third of the patients have been operated in 2018. When neurosurgical operative microscope was not available, ophthalmologic microscope or binocular with headlight were used to achieve the resection. Pathological examination revealed High-grade glioma, subependymal giant cell astrocytoma (SEGA), central neurocytoma, Subependymoma, Hemangioblastoma, pilocytique astrocytoma, Medulloblastoma, gemiocytic astrocytoma, atypical papilloma of choroid plexus, craniopharygioma and cyst of septum pellucidum. We reported good postoperative outcome in 10 cases (66.6%), moderate postoperative deficit in 1 case and 4 cases of postoperative death (26.6%) among which 3 cases of postoperative meningitis. Conclusion: Periventricular and intraventricular processes can be safely approach in low-income country with acceptable result. However young African Neurosurgeon should be trained to be comfortable with multiple surgical approaches and also with binocular as well as with microscope. WFNS training program is a strong basement for the take-off of young African neurosurgeon. Backing home should be the rule after training, to develop neurosurgery.
| Published in | International Journal of Neurosurgery (Volume 8, Issue 1) |
| DOI | 10.11648/j.ijn.20240801.11 |
| Page(s) | 1-10 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Periventricular, Intraventricular, Tumor, Process, WFNS Rabat Training Center Program
Age: Year | Year of surgery | Symptome | Tumor Location | Approach | Preoperative shunting | |
|---|---|---|---|---|---|---|
1 | 12 | 2015 | ICH + cerebellar syndrome | V4 (and floor of V4 | Telovelar | No |
2 | 4 | 2017 | ICH + cerebellar syndrome | (cerebellar) V4 | Trans cerebellar | VPS |
3 | 17 | 2017 | ICH + cerebellar syndrome | (cerebellar V4) | Trans cerebellar | VPS |
4 | 29 | 2018 | ICH | Right V2 (extended to left thalamus | Left transfrontal | No |
5 | 4 | 2018 | ICH + cerebellar syndrome | (Cerebellar) V4 | Trans cerebellar | VPS |
6 | 5 | 2018 | ICH + cerebellar syndrome | V4 (and floor of V4) | Telovelar | Ventriculo cisternostomy |
7 | 27 | 2018 | ICH + cerebellar syndrome | V4 | Telovelar | VPS |
8 | 14 | 2018 | ICH + hemiparesis (2/5) | Thalamus | Endoscopic removal of the nodule | No |
9 | 6 | 2019 | ICH | Left Monro (V2) | left inter hemispheric | VPS |
10 | 30 | 2020 | Headache | Thalamus | Controlateral inter hemispheric | No |
11 | 23 | 2020 | ICH | Left V2 (atrium) | Transtemporal (Trans T2) | No |
12 | 6 | 2020 | ICH | suprasellar extended to V3 | Subfrontal transbasal translamina terminalis | VPS |
13 | 38 | 2021 | ICH + cerebellar syndrome | cerebellar extended to V4 | Trans cerebellar | VPS |
14 | 39 | 2022 | ICH + Coma | V2 (septum pellicidum | Cysto peritoneal shunting | Not applicable |
15 | 35 | 2023 | ICH | V4 | Telovelar | No |
surgical duration | tumor removal | Postoperative outcome | Pathological examination | Recurrence | Alive at One year follow up | |
|---|---|---|---|---|---|---|
1 | 11 | Subtotal | Improved then meningitis and death at 2 month | Gemiocytic astrocytoma | Not applicable | No |
2 | 11 | Total | Meningitis and death | Pilocytic astrocytoma | Not applicable | No |
3 | 15 | Total | Improved | Pilocytic astrocytoma | No | Yes |
4 | 14 | subtotal | Right hemiparesis | Central neurocytoma | Yes (3 more surgery) | Yes |
5 | 11 | Total | Improved | hemangioblastoma | No | Yes |
6 | 13 | Subtotal | Postoperative mortality (respiratory distress) | Medulloblastoma (grade IV WHO) | Not applicable | No |
7 | 15 | Total | Improved | Atypic papilloma of choroid plexus | No | Yes |
8 | 5 | Total | Improved | Pilocytic astrocytoma | No | Yes |
9 | 10 | subtotal | Improved | SEGA (subependymal giant cell astrocytoma) | No | Yes |
10 | 12 | Subtotal | Improved | Fibrillary astrocytoma | Progression to High grade glioma (adjuvant treatment Stupp protocol) | Yes (death at post operative 14th month) |
11 | 8 | subtotal | improved | sub ependymoma | Yes (total removal after the recurrence) | Yes |
12 | 16 | Total | improved | Craniopharyngioma | No | Yes |
13 | 11 | Total | improved | Hemangioblastoma | No | yes |
14 | 1 | Shunting | Improved | Possible arachnoid cyst on CT Scan | No | Yes |
15 | 13 | Subtotal | Improved then ventriculis and death | Epidermoid cyst | Not applicable | No |
| [1] | Elwatidy S. M, Al Towin A. A, Malick S. H. tumors of lateral and third ventricle: surgical management and outcome analysis in 42 cases. Neurosciences. 2017; 22 (4): 274-281. |
| [2] |
Lim J, Park Y, Ahn JW, Hwang SJ, Kwon H, Sung S K, Cho K. Maximal surgical resection and adjuvant surgical technique to Prolong the survival of adult patients with thalamic glioblastoma. PLoS One. 2021; 16 (2): E0244325
https://doi.org/10.1371/journal.pone.0244325.eCollection2021 |
| [3] | Principles of intraventricular surgery. Neurosurgical atlas. |
| [4] | Karekezi C, El Khamlichi A, El Ouahabi A, El Abbadi N, Ahokpossi SA, Ahanogbe KMH, Berete I, Bouya SM, Coulibaly O, Dao I, Djoubairou BO, Doleagbenou AAK, Egu KP, Mbaki HBE, Kinata-Bambino SB, Habibou LM, Mousse AN, Ngamasata T, Ntalaja J et al (2020) The impact of African-trained neurosurgeons on sub-Saharan Africa. Neurosurg Focus. 48(3): E4. |
| [5] | Megerssa TB, Mahesparan R. Surgical Outcome of Intraventricular Tumors; A Retrospective Single Center Study in Addis Ababa, Ethiopia. SVOA Neurology. 2024; 5: 1: 26-36. |
| [6] | Filippidis A, Tsonidis CA. Intraventricular brain tumors in children. Pediatr Neurosurg. 1989; 5: 230-233. |
| [7] | Ellenbogen RG. Transcortical surgery for lateral ventricular tumors. FOC. 2001; 10 (6): 1-13. |
| [8] | Kasowski H, Piepmeier JM. Transcallosal approach for tumors of the lateral and third ventricles. FOC. 2001; 10(6): 1- 5. |
| [9] | Kriankumar C, Deshpande R, K. Chandrasekhar YbV, Rao Is, Panigrahi M, Babu P. Clinical management and prognostic outcome of intracranial ventricular tumors: A study of 134 cases. Cancer Res Stat Treat. 2019; 2(1): 10. |
| [10] | Vigo, V., Monroy-Sosa, A., Rodriguez-Rubio, R. (2021). Surgical Treatment of Intraventricular Tumors. In Brain and Skull Base, (eds) Principles of Neuro-Oncology. Switzerland: Springer Nature, Cham; 2021, 561-581 |
| [11] | Grundy P, Apostolopoulos V. Intraventricular tumors. In: Kirollos AH RW, Thomson S, Hutchinson PJA, editors. Neurological surgery: Oxford University Press; 2019. |
| [12] | Yasargil MG, Abdulrauf SI. Surgery of intraventricular tumors. Neurosurgery. 2008; 62 (6 Suppl 3): 1029–40. discussion 40-1. |
| [13] | Zanini MA, Faleiros AT, Almeida CR, Clara CA, Gabarra RC. Trigone ventricular meningiomas: surgical approaches. Arq Neuropsiquiatr. 2011; 69 (4): 670–675. |
| [14] | For the French Society of Neurosurgery, Lubrano V, François P, Loundou A, Vasiljevic A, Roche PH. Outcomes after surgery for central neurocytoma: results of a French multicentre retrospective study. Acta Neurochir. 2013; 155 (7): 1261-1269. |
APA Style
Dao, I., Kièmtoré, A., Ouattara, O., Bako, F., Traoré, J., et al. (2024). Periventricular and Intraventricular Tumors in a Low-Income Country: Hard Learning Curve and Outcome of a Young Neurosurgeon from Burkina Faso. International Journal of Neurosurgery, 8(1), 1-10. https://doi.org/10.11648/j.ijn.20240801.11
ACS Style
Dao, I.; Kièmtoré, A.; Ouattara, O.; Bako, F.; Traoré, J., et al. Periventricular and Intraventricular Tumors in a Low-Income Country: Hard Learning Curve and Outcome of a Young Neurosurgeon from Burkina Faso. Int. J. Neurosurg. 2024, 8(1), 1-10. doi: 10.11648/j.ijn.20240801.11
@article{10.11648/j.ijn.20240801.11,
author = {Ibrahim Dao and Aminata Kièmtoré and Ousmane Ouattara and Frédéric Bako and Jacques Traoré and Joseph Biogo and Serge Pacôme Yameogo and Abdoulaye Sanou and Eustache Kienou and Louis Junior Comboigo and Arsène Tossou and Abdoulaye Thiombiano and Lassané Taoko and Henry Lankoandé and Elie Nassoum and Narcisse Ouédraogo and Sosthène Fawaz Adéniran and Astride Somda and Delwendé Sylvain Zabsonré and Abel Kabré},
title = {Periventricular and Intraventricular Tumors in a Low-Income Country: Hard Learning Curve and Outcome of a Young Neurosurgeon from Burkina Faso
},
journal = {International Journal of Neurosurgery},
volume = {8},
number = {1},
pages = {1-10},
doi = {10.11648/j.ijn.20240801.11},
url = {https://doi.org/10.11648/j.ijn.20240801.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20240801.11},
abstract = {Background: Periventricular and Intraventricular processes are life-threatening conditions because of their propensity to obstruct Cerebrospinal fluid pathways and to compress highly functional and vital structures. There are deep-seated lesions requiring rigorous microsurgical technic for their resection. Methods: We retrospectively analyzed the profile and outcome of Periventricular and intraventricular processes operated by the same author since his return in his country in 2015, after graduated abroad in WFNS Rabat training center program 2023. Result: We defined 15 patients operated over 8 years. There were 4 processes in lateral ventricle (26.6%), 1 in third ventricle (6.6%), 2 thalamus processes (13.3%), 4 in fourth ventricle (26.6%) and finally 4 in cerebellar hemisphere and violating the fourth ventricle (26.6%). Various surgical approaches were used, such as contralateral interhemispheric transcallosal, classical interhemispheric transcallosal, Subfrontal transbasal translamina terminalis, Frontal Transcortical, Temporal trans T2, ventriculoperitoneal shunting, endoscopy, cerebellar transcotical approach and Telovelar approach. Surgical procedure duration was more than 10 hours in 12 cases (80%) and one third of the patients have been operated in 2018. When neurosurgical operative microscope was not available, ophthalmologic microscope or binocular with headlight were used to achieve the resection. Pathological examination revealed High-grade glioma, subependymal giant cell astrocytoma (SEGA), central neurocytoma, Subependymoma, Hemangioblastoma, pilocytique astrocytoma, Medulloblastoma, gemiocytic astrocytoma, atypical papilloma of choroid plexus, craniopharygioma and cyst of septum pellucidum. We reported good postoperative outcome in 10 cases (66.6%), moderate postoperative deficit in 1 case and 4 cases of postoperative death (26.6%) among which 3 cases of postoperative meningitis. Conclusion: Periventricular and intraventricular processes can be safely approach in low-income country with acceptable result. However young African Neurosurgeon should be trained to be comfortable with multiple surgical approaches and also with binocular as well as with microscope. WFNS training program is a strong basement for the take-off of young African neurosurgeon. Backing home should be the rule after training, to develop neurosurgery.
},
year = {2024}
}
TY - JOUR T1 - Periventricular and Intraventricular Tumors in a Low-Income Country: Hard Learning Curve and Outcome of a Young Neurosurgeon from Burkina Faso AU - Ibrahim Dao AU - Aminata Kièmtoré AU - Ousmane Ouattara AU - Frédéric Bako AU - Jacques Traoré AU - Joseph Biogo AU - Serge Pacôme Yameogo AU - Abdoulaye Sanou AU - Eustache Kienou AU - Louis Junior Comboigo AU - Arsène Tossou AU - Abdoulaye Thiombiano AU - Lassané Taoko AU - Henry Lankoandé AU - Elie Nassoum AU - Narcisse Ouédraogo AU - Sosthène Fawaz Adéniran AU - Astride Somda AU - Delwendé Sylvain Zabsonré AU - Abel Kabré Y1 - 2024/04/17 PY - 2024 N1 - https://doi.org/10.11648/j.ijn.20240801.11 DO - 10.11648/j.ijn.20240801.11 T2 - International Journal of Neurosurgery JF - International Journal of Neurosurgery JO - International Journal of Neurosurgery SP - 1 EP - 10 PB - Science Publishing Group SN - 2640-1959 UR - https://doi.org/10.11648/j.ijn.20240801.11 AB - Background: Periventricular and Intraventricular processes are life-threatening conditions because of their propensity to obstruct Cerebrospinal fluid pathways and to compress highly functional and vital structures. There are deep-seated lesions requiring rigorous microsurgical technic for their resection. Methods: We retrospectively analyzed the profile and outcome of Periventricular and intraventricular processes operated by the same author since his return in his country in 2015, after graduated abroad in WFNS Rabat training center program 2023. Result: We defined 15 patients operated over 8 years. There were 4 processes in lateral ventricle (26.6%), 1 in third ventricle (6.6%), 2 thalamus processes (13.3%), 4 in fourth ventricle (26.6%) and finally 4 in cerebellar hemisphere and violating the fourth ventricle (26.6%). Various surgical approaches were used, such as contralateral interhemispheric transcallosal, classical interhemispheric transcallosal, Subfrontal transbasal translamina terminalis, Frontal Transcortical, Temporal trans T2, ventriculoperitoneal shunting, endoscopy, cerebellar transcotical approach and Telovelar approach. Surgical procedure duration was more than 10 hours in 12 cases (80%) and one third of the patients have been operated in 2018. When neurosurgical operative microscope was not available, ophthalmologic microscope or binocular with headlight were used to achieve the resection. Pathological examination revealed High-grade glioma, subependymal giant cell astrocytoma (SEGA), central neurocytoma, Subependymoma, Hemangioblastoma, pilocytique astrocytoma, Medulloblastoma, gemiocytic astrocytoma, atypical papilloma of choroid plexus, craniopharygioma and cyst of septum pellucidum. We reported good postoperative outcome in 10 cases (66.6%), moderate postoperative deficit in 1 case and 4 cases of postoperative death (26.6%) among which 3 cases of postoperative meningitis. Conclusion: Periventricular and intraventricular processes can be safely approach in low-income country with acceptable result. However young African Neurosurgeon should be trained to be comfortable with multiple surgical approaches and also with binocular as well as with microscope. WFNS training program is a strong basement for the take-off of young African neurosurgeon. Backing home should be the rule after training, to develop neurosurgery. VL - 8 IS - 1 ER -
Department of Orthopaedic Surgery, Souro Sanou University Hospital, Bobo Dioulasso, Burkina Faso; Military Hospital Colonel Major Tanguet Ouattara, Bobo Dioulasso, Burkina Faso; Higher Institute of Health Sciences, Nazi Boni University, Bobo Dioulasso, Burkina Faso
Biography: Ibrahim Dao is an assistant professor in neurosurgery at the Higher Institute of Health Sciences in Bobo Dioulasso (Nazi Boni University) since 2019. He holds also the position of neurosurgeon at the University Hospital Souro Sanou and at the Military Hospital Colonel Major Tanguet Ouattara.
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Orthopaedic Surgery, Souro Sanou University Hospital, Bobo Dioulasso, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Orthopaedic Surgery, Souro Sanou University Hospital, Bobo Dioulasso, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso
Department of Neurosurgery, Yalgado Ouedraogo University Hospital, Joseph KI-Zerbo University, Ouagadougou, Burkina Faso

Figure 1. (case 10 in the table): Preoperative images: left thalamic glioma.

Figure 2. (Case 10 in the table): Intraoperative images of left thalamic process: Interhemispheric contralateral approach: position (A), Opening of dura matter (B), interhemispheric approach with exposition of the corpus callosum (C), Callosotomy then exposition of the left thalamus and thalamostriate vein (D), resection cavity (D: white arrow).

Figure 3. (case 10 in the table): Postoperative images: left thalamic glioma (Noticed the resection cavity: white star).
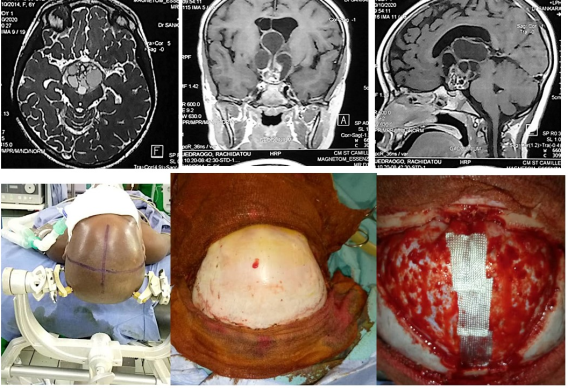
Figure 4. (Case 12 in the table): Suprasellar craniopharyngioma extended to V3. Subfrontal transbasal translamina terminalis approach (Middle line images).
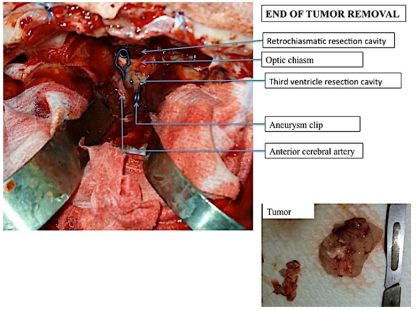
Figure 5. (Case 12 in the table): Suprasellar craniopharyngioma extended to V3: intraoperative view after complete removal: incidental rupture of anterior communicating artery (Clipped).

Figure 6. (Case 12 in the table): Suprasellar craniopharyngioma extended to V3 (Upper line images) Post operative control: Total removal and patency of Willis circle.

Figure 7. (Case 7 in the table): Atypic papilloma of choroid plexus of V4: Complete removal through telovelar approach: Note the floor of V4 at the end of the surgery.

Figure 8. Our practice: Surgery with neurosurgical microscope (A); Posterior fossa approach for a resection of an hemangioblastoma with binocular when microscope was unavailable (B); Training with chicken wing and binocular with headlight (C).
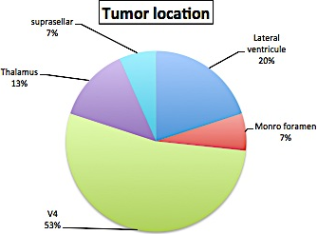
Figure 9. Tumor location.

Figure 10. Surgical duration.

